
An ACL (anterior cruciate ligament) injury is one of the most serious knee injuries in football (soccer). The ACL is a key ligament inside the knee that stabilizes the joint, preventing the shin bone (tibia) from sliding too far forward under the thigh bone (femur). Footballers who tear this ligament often hear a “pop” and experience immediate swelling and pain. Such injuries usually require surgery and a long rehabilitation period. Understanding what the ACL does and how it can get injured helps players appreciate the need for careful treatment and rehab.
Understanding the ACL Injury
The ACL is one of four major ligaments in the knee and it crosses diagonally to connect the femur (thigh bone) to the tibia. It controls how far forward the tibia can move relative to the femur, keeping the knee stable during cutting or pivoting moves. In football, ACL tears often happen during sudden stops, rapid direction
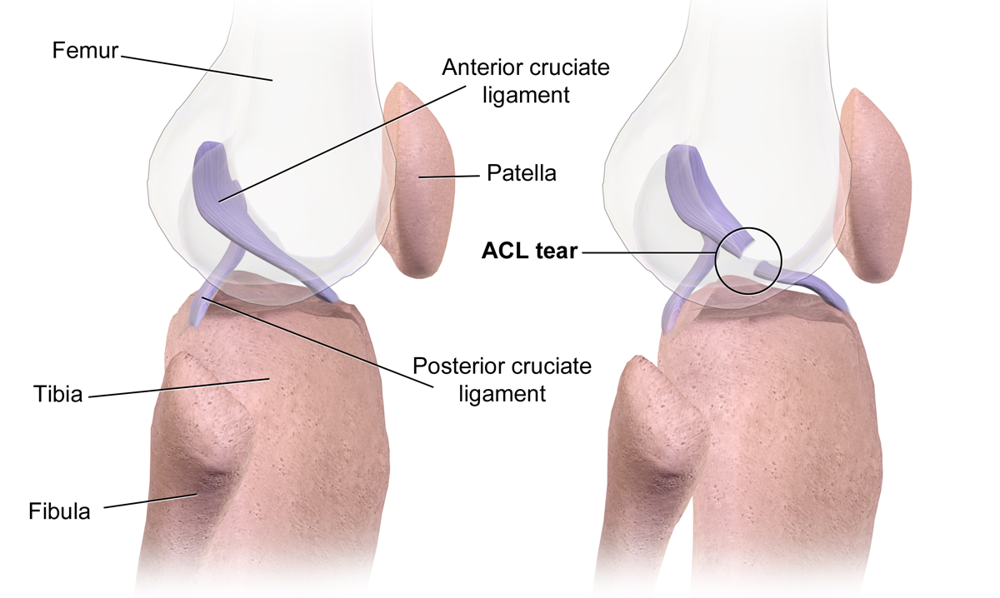
changes, or awkward landings. When the ACL tears, players typically feel or hear a “pop” and the knee rapidly swells from bleeding within the joint. This blood usually appears within an hour or two. Other classic signs are severe pain, inability to keep playing, and a feeling that the knee is unstable or “giving way.” If unchecked, this instability can lead to further knee damage. Prompt diagnosis is key; a doctor will examine the knee and usually get an MRI to confirm the tear.
Immediate Steps After Injury
Right after an ACL injury, quick care can help. Follow the RICE protocol (Rest, Ice, Compression, Elevation) to control swelling and pain. This means immediately resting the injured knee, applying ice packs, using a compression bandage or wrap, and keeping the leg elevated above heart level. Keep weight off the knee – use crutches if needed – until a doctor evaluates it. Early bracing (a knee support) may be used to stabilize the knee if there is doubt about the tear. As soon as possible, see a healthcare professional: they will check the knee, control pain, and discuss whether imaging or specialist care is needed. Over-the-counter pain medicines (like acetaminophen) can help, but avoid anti-inflammatory pills if the doctor advises waiting for an evaluation. Keeping the knee slightly bent (about 30–90 degrees) may be more comfortable and can help prevent stiffness.
Surgery and What to Expect
Most athletes with a complete ACL tear will undergo surgical reconstruction, especially footballers who need a stable knee for sport. Surgery is done arthroscopically (with small incisions) to replace the torn ligament. The surgeon usually uses a graft (a piece of tendon tissue) from the patient’s own body (autograft) – often the middle third of the patellar tendon or the hamstring tendons – to form a new ligament. (A graft is essentially replacement tissue used to recreate the torn ligament.) Sometimes a quadriceps tendon graft is used, or donor tissue in special cases. The graft is fixed into place with screws or plugs so it holds the bones in alignment.
You will likely go home the same day or the next, depending on surgeon and any other repairs done (e.g. meniscus repair may require one night). Expect to start physical therapy immediately after surgery. In fact, patients usually begin gentle exercises on the day of surgery, even in the recovery room. Initially the knee may be braced in extension to protect the graft; many surgeons, however, allow early motion and do not require a long-term brace. You will go home with crutches. Most patients are comfortable enough to walk without crutches in about 7–10 days, assuming no other knee repairs were done. In the first week or two, the main goals are to control pain and swelling, straighten (fully extend) the knee again, and activate the quadriceps muscles. You will ice frequently and may use a CPM machine (continuous passive motion) or stationary bike at low resistance to gently move the knee.
Hospital Follow-up: You will usually have a check-up with the surgeon around 1–2 weeks after surgery, then at 6 weeks, 3 months, and later to track progress. These visits ensure the knee is healing (no infection or complications), measure range of motion, and assess strength gains. Full recovery does take many months, but careful step-by-step rehab maximizes success.
Recovery Timeline (Month-by-Month Milestones)
Rehabilitation is gradual. Below is a general guide; individual pace can vary. Progress through these phases under professional guidance:
Month 1 (Weeks 1–4): Focus on healing. Swelling control and extension are priorities. Continue RICE, keep the knee elevated as much as possible, and do gentle exercises (ankle pumps, straight-leg raises, glute squeezes) to prevent stiffness. By the end of the first month, work on achieving full extension (straightening the knee) and bending to about 90° flexion. Light exercises like stationary cycling (no resistance) help keep motion without overloading the knee. Proper nutrition, hydration, and rest also support healing in this early stage.
Month 2 (Weeks 5–8): The graft is maturing (remodeling into a new ligament). Pain and swelling should greatly improve. Patients typically wean off crutches early in this phase. You can gradually increase range of motion exercises and begin gentle weight-bearing strengthening. Physical therapy will introduce exercises like mini-squats (partial knee bends), heel slides (bending the knee while sliding heel on floor), and low-resistance leg presses. Balance and core stability work may begin. By 6–8 weeks, many patients can walk normally without a limp as strength improves.
Month 3 (Weeks 9–12): The knee is stronger and can handle more loading. Continue to build knee flexion (aim for near-normal bend). Advance strengthening: progress closed-chain exercises (e.g. squats, lunges, step-ups) and add straight-leg raise variations. Gym bike and elliptical trainers can increase intensity. Functional exercises – like step-downs and resisted hamstring curls – are typical. The focus is on strengthening and neuromuscular control. By 3 months, you should have good control doing bodyweight moves; your therapist may begin introducing light jogging form drills on soft ground (but high-impact running/jumping usually waits).
Month 4–6: Now training can include more dynamic activities. The reconstructed ligament has grown stronger with bone integration of the graft. We introduce running (starting with straight-line jogging, then gradual cutting and sprint drills), plyometrics (short jumps/landings with focus on good form), and agility drills (direction changes). Emphasis is placed on perfecting jumping and landing technique to protect the knee – for example, landing softly with knees aligned, avoiding inward collapse of the knee (valgus position). By 6 months, goals typically include running without pain, performing single-leg hops, and full participation in gym exercises (squats, deadlifts, agility drills).
Month 6–12: Return to play readiness. If strength, stability, and functional tests are excellent (e.g. single-leg hop tests, strength symmetry ≥90%), many players are cleared to return to football at 6–9 months. However, healing continues past 6 months, and some athletes take 9–12 months or more to feel completely ready. Ongoing training should be progressive: full training drills without contact, then non-contact practice, and finally full contact in games. At this stage, a doctor or therapist often performs tests (strength, jumping, agility) to give a green light.
Physiotherapy and Rehab Exercises
Physical therapy is the cornerstone of ACL recovery. A physiotherapist will guide a structured program that safely advances week by week. Early on (weeks 0–4), focus on regaining full knee extension and activating the quadriceps. This may include exercises like straight-leg raises, quadriceps sets (tightening the thigh muscle with knee straight), and gentle range-of-motion exercises. Stationary cycling at no resistance is often used to encourage safe movement. Patience is key: forcing deep bends too early can irritate the knee. As swelling subsides and

strength builds (months 2–3), the program adds closed-chain strengthening – meaning exercises where the foot stays on a surface. Examples are mini-squats, wall sits, leg presses, and step-ups. These safely load the knee muscles without stressing the ligament graft. Balance and proprioception (joint sense) exercises are added, such as single-leg
stands on stable then unstable surfaces (balance boards). This retrains the knee’s reflex control. Later (months 3–6+), therapy incorporates sport-specific drills: single-leg hopping, box jumps, lunges with rotation, and cutting maneuvers, all focusing on proper alignment and muscle coordination. Functional exercises like hamstring curls and hip bridges ensure the posterior muscles (hamstrings, glutes) become as strong as the quads, which is crucial for knee stability. Throughout rehab, exercise difficulty, repetitions, and resistance are increased gradually, always monitoring pain and swelling. It is important to follow the therapist’s guidance to avoid setbacks and to reach full strength safely.
Nutrition for Healing
Good nutrition speeds healing. Emphasize protein-rich foods (chicken, fish, lean beef, eggs, dairy, beans) because protein is the building block of muscle and ligament repair. Vitamins and minerals from fruits and vegetables are also important: for example, vitamin C (found in citrus fruits, berries) helps collagen formation in tissues, and other vitamins (A, D, K, E) support overall recovery. Foods high in omega-3 fatty acids (such as salmon, walnuts, flaxseed) have anti-inflammatory effects and support healing. Hydration is often overlooked but crucial – drink plenty of water to aid tissue repair and reduce swelling.
Supplements can help if diet lacks certain nutrients. A joint-support supplement with collagen or vitamin C may assist ligament healing (since the ACL is mostly connective tissue). A multivitamin can provide essential vitamins (C, D, etc.) and minerals (zinc, calcium) needed during recovery. On the other hand, avoid excess junk food or alcohol: processed foods offer little nutrition, and alcohol can impede healing (it thins blood and dehydrates). Overall, a balanced, nutrient-dense diet with focus on healing foods will give the body the resources it needs to rebuild the knee.
Mental Recovery and Motivation
Recovering from ACL surgery is as much a mental challenge as a physical one. Players often experience frustration, sadness, or fear of getting hurt again. It’s common to feel depressed or anxious during the long rehab process. Acknowledge these feelings: they are a normal response to injury. Setting small, attainable goals (e.g. bend the knee a little more each week) helps maintain motivation. Keeping a positive mindset and visualizing successful recovery can also help.
Staying connected to the team and sport in other ways (reviewing game footage, doing light upper-body workouts, watching practice) keeps the spirit engaged. Many athletes find it helpful to lean on family, teammates, or a sports psychologist for support. If anxiety or depression become severe, professional help should be sought, as psychological health greatly impacts physical recovery. Celebrate the milestones – each new degree of motion or strength gain – and remember that consistent effort leads to progress. In the end, a patient, goal-oriented mindset will carry you through the hardest months.
Returning to Football Safely
Coming back to football must be done carefully to prevent re-injury. Before full return, the knee should be nearly back to normal strength and function. Doctors and therapists typically require no swelling, full range of motion, and strength tests met (often >90% of the uninjured leg) before
clearance. Functional tests – like single-leg hops, shuttle runs, and agility drills – are used to confirm stability. Only when you can comfortably squat, lunge, and hop without pain or wobbling will you be allowed to resume full training. Even then, a gradual progression is best. Start with non-contact drills in practice (passing, shooting, running on the pitch) and

ensure you can perform them safely. Then move to controlled scrimmages, and finally full games. Some players wear a knee brace or kinesiology tape on game days for extra support and confidence, especially in the first year, although evidence is mixed on performance benefit. Communicate with coaches and trainers; if the knee feels unstable or swollen after training, scale back intensity and consult your medical team. Ultimately, combining objective recovery criteria with smart training ensures the safest comeback.
Prevention Tips for the Future
Preventing future ACL injuries involves training and caution. Incorporate neuromuscular training (exercise programs that improve control and alignment) into regular workouts. Studies show that balance and agility drills – such as single-leg balance exercises, plyometrics (jump training), and agility courses – can improve knee control and reduce ACL risk. Many teams use programs like FIFA 11+ (dynamic warm-up routines focused on strength, balance, and plyometrics) to prevent injuries. Strengthening the leg muscles around the knee is key: strong hamstrings and glute muscles help protect the ACL by controlling the thigh bone’s motion.
Always warm up properly before training and games, and emphasize landing safely from jumps (land with knees bent and aligned over feet, not caving inward). Avoid playing when fatigued or on very uneven surfaces, as tired muscles can’t protect the knee as well. Learn and practice good techniques (e.g. pivot by lifting the foot instead of planting a straight leg and twisting). Over time, these habits and training drills build knee resilience. By keeping the muscles strong and the nervous system sharp, you greatly lower the chance of re-injury and stay on the pitch for the future.